 Adobe PDF
Adobe PDF
 Microsoft Word
Microsoft Word
 OpenDocument
OpenDocument
Regulations
There are no country-wide requirements for using an employee emergency contact form. Employers are recommended to verify local rules and industry-specific regulations.
Sample
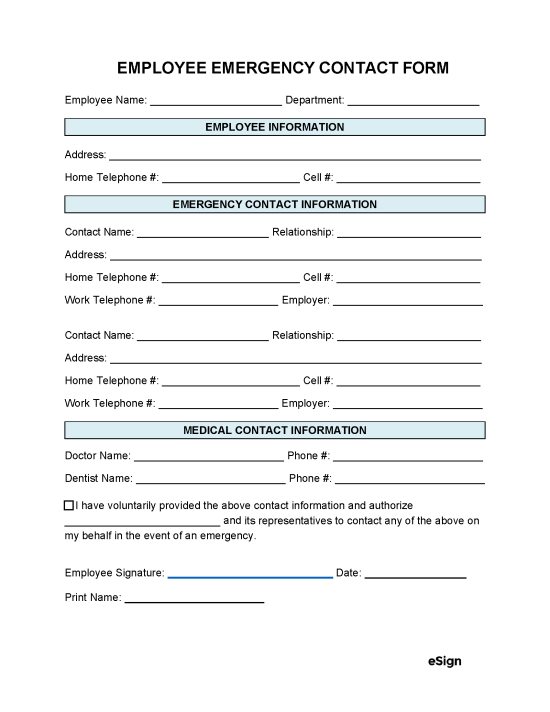
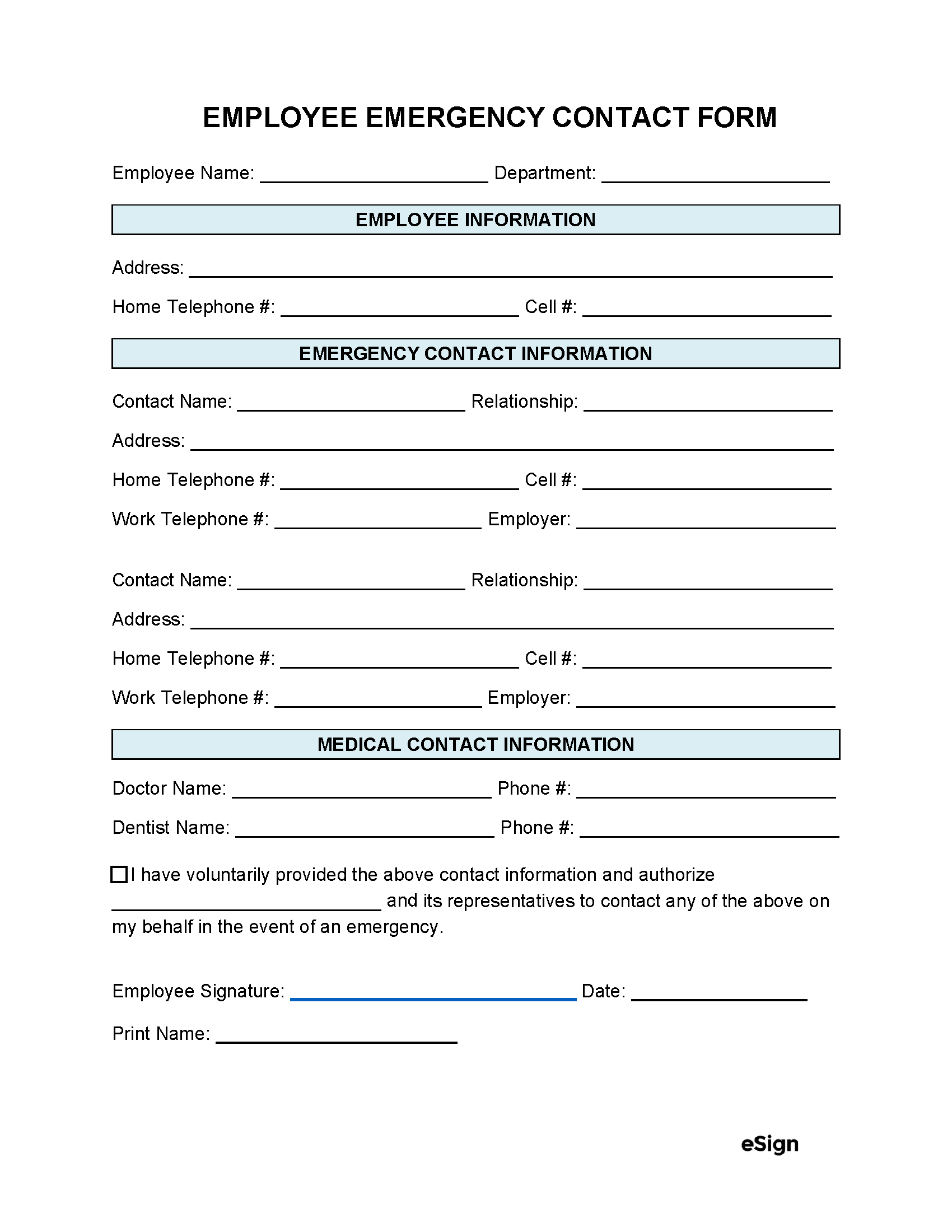
EMPLOYEE EMERGENCY CONTACT FORM
Employee Name: [EMPLOYEE NAME] Department: [EMPLOYEE DEPARTMENT]
EMPLOYEE INFORMATION
Address: [EMPLOYEE ADDRESS]
Home Telephone #: [EMPLOYEE HOME PHONE #] Cell #: [EMPLOYEE CELL PHONE #]
EMERGENCY CONTACT INFORMATION
Contact Name: [CONTACT NAME] Relationship: [CONTACT RELATIONSHIP]
Address: [CONTACT ADDRESS] Home Telephone #: [CONTACT HOME PHONE #]
Cell #: [CONTACT CELL PHONE #] Work Telephone #: [CONTACT WORK PHONE #]
Employer: [CONTACT EMPLOYER]
Contact Name: [CONTACT NAME] Relationship: [CONTACT RELATIONSHIP]
Address: [CONTACT ADDRESS] Home Telephone #: [CONTACT HOME PHONE #]
Cell #: [CONTACT CELL PHONE #] Work Telephone #: [CONTACT WORK PHONE #]
Employer: [CONTACT EMPLOYER]
MEDICAL CONTACT INFORMATION
Doctor Name: [DOCTOR NAME] Phone #: [DOCTOR PHONE #]
Dentist Name: [DENTIST NAME] Phone #: [DENTIST PHONE #]
☐ I have voluntarily provided the above contact information and authorize [EMPLOYER NAME] and its representatives to contact any of the above on my behalf in the event of an emergency.
Employee Signature: Date: ______________
Print Name: [EMPLOYEE NAME]