 Adobe PDF
Adobe PDF
 Microsoft Word
Microsoft Word
 OpenDocument
OpenDocument
Getting the customer’s approval with the form helps build trust and improves the likelihood that a merchant wins a dispute in the event of a chargeback. Using a physical authorization form is commonplace among brick-and-mortar establishments, as digital (software) companies typically require the customer to confirm their understanding of the terms and conditions at checkout. To avoid fraud and/or stolen customer information, merchants must ensure all authorization forms are stored securely and can only be accessed by employees with a valid reason for viewing the data.
Sample
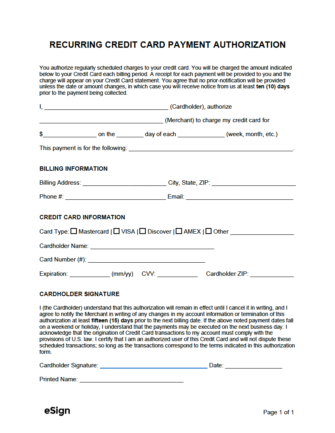
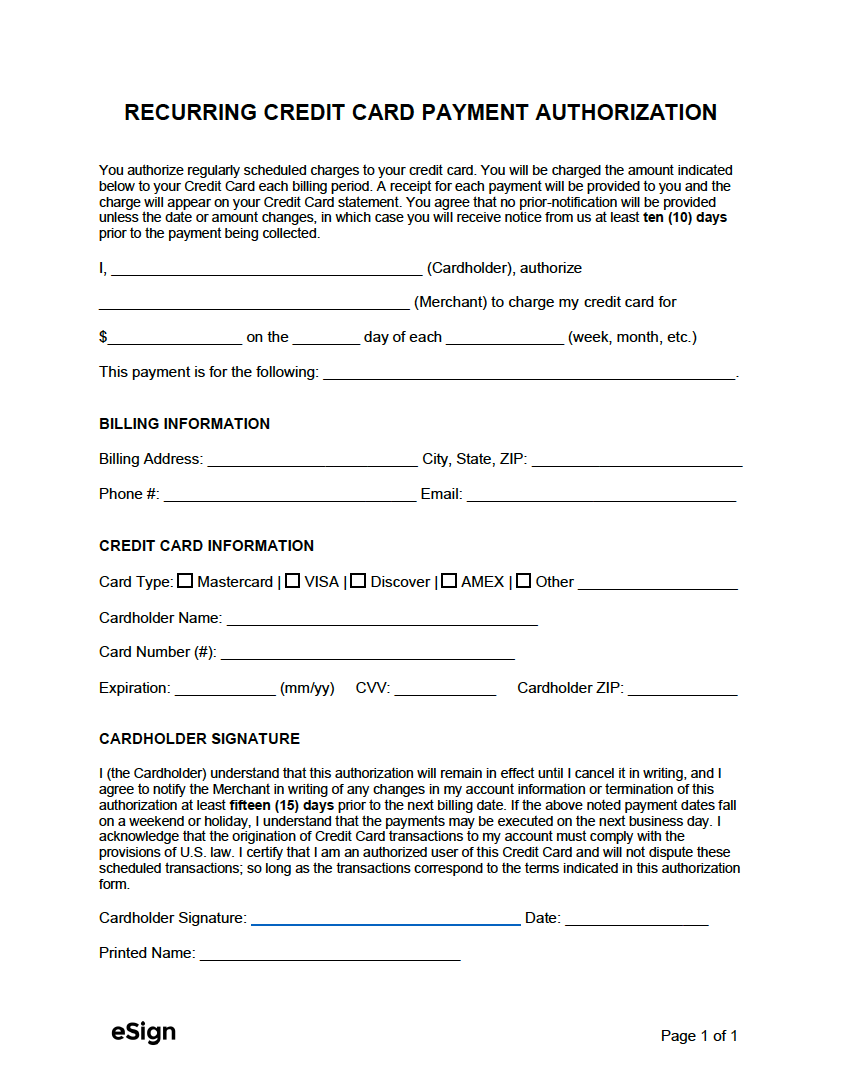
RECURRING CREDIT CARD PAYMENT AUTHORIZATION
You authorize regularly scheduled charges to your credit card. You will be charged the amount indicated below to your Credit Card each billing period. A receipt for each payment will be provided to you, and the charge will appear on your Credit Card statement. You agree that no prior notification will be provided unless the date or amount changes, in which case you will receive notice from us at least ten (10) days before the payment is collected.
I, [CARDHOLDER NAME], authorize [MERCHANT NAME] to charge my credit card for $[AMOUNT] on the [#] day of each [FREQUENCY] (week, month, etc.)
This payment is for the following: [REASON FOR PAYMENT].
BILLING INFORMATION
Billing Address: [STREET ADDRESS] City, State, ZIP: [CITY, STATE, & ZIP]
Phone #: [CARDHOLDER PHONE] Email: [CARDHOLDER EMAIL]
CREDIT CARD INFORMATION
Card Type: ☐ Mastercard | ☐ VISA | ☐ Discover | ☐ AMEX | ☐ Other [OTHER]
Cardholder Name: [CARDHOLDER NAME]
Card Number (#): [CREDIT CARD #]
Expiration: [MM/YY] CVV: [CVV #] Cardholder ZIP: [ZIP CODE]
CARDHOLDER SIGNATURE
I (the Cardholder) understand that this authorization will remain in effect until I cancel it in writing. I agree to notify the Merchant in writing of any changes in my account information or termination of this authorization at least fifteen (15) days before the next billing date. If the above-noted payment dates fall on a weekend or holiday, I understand that the payments may be executed on the next business day. I acknowledge that the origination of Credit Card transactions to my account must comply with the provisions of U.S. law. I certify that I am an authorized user of this Credit Card and will not dispute these scheduled transactions; so long as the transactions correspond to the terms indicated in this authorization form.
Cardholder Signature: ________________________________ Date: [MM/DD/YYYY]
Printed Name: [CARDHOLDER PRINTED NAME]