 Adobe PDF
Adobe PDF
 Microsoft Word
Microsoft Word
 OpenDocument
OpenDocument
Common Uses
- Workplace – Employee discrimination, harassment, safety hazards, and accidents.
- Police – Vandalism, theft, assault, and other criminal activity requiring investigation.
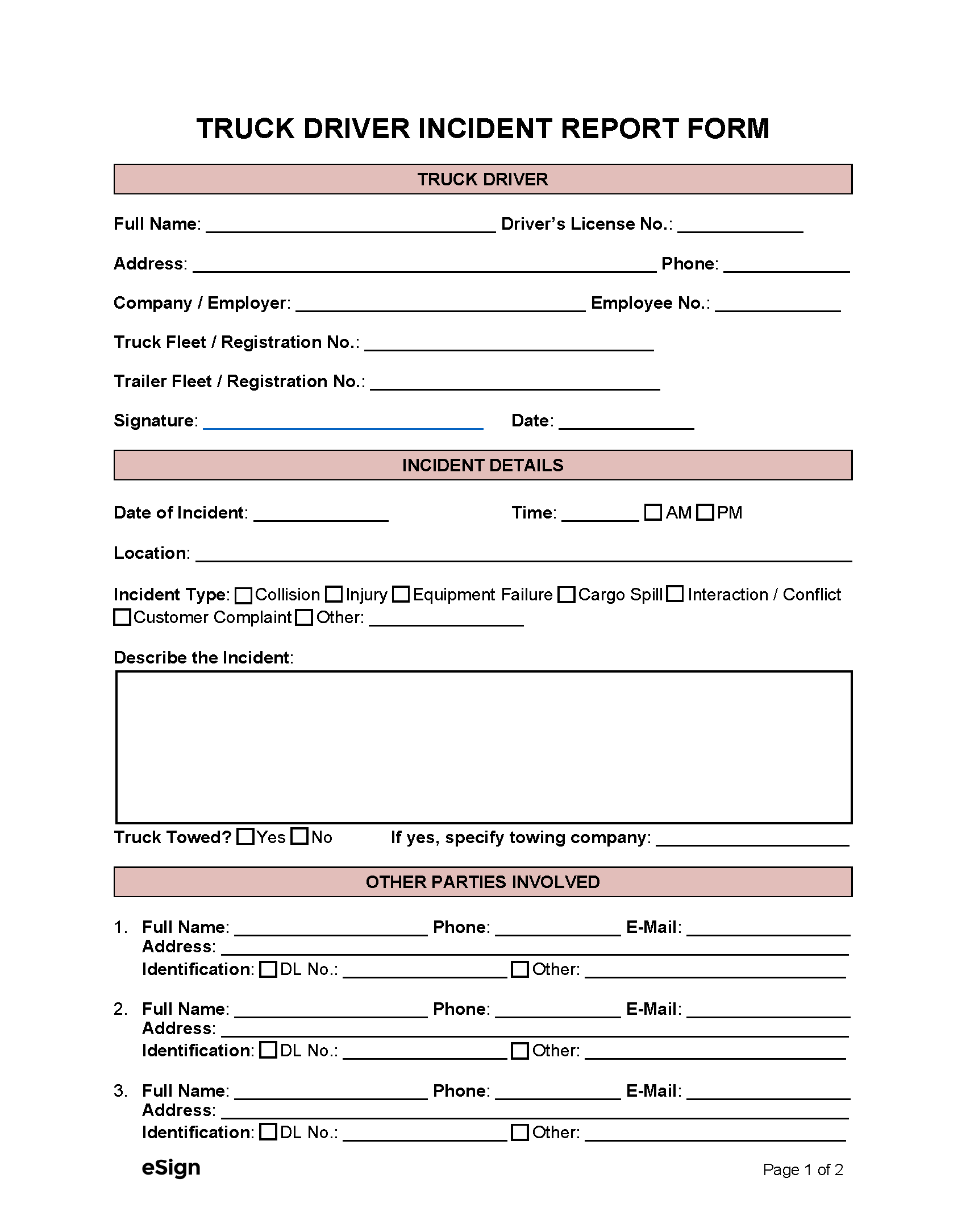
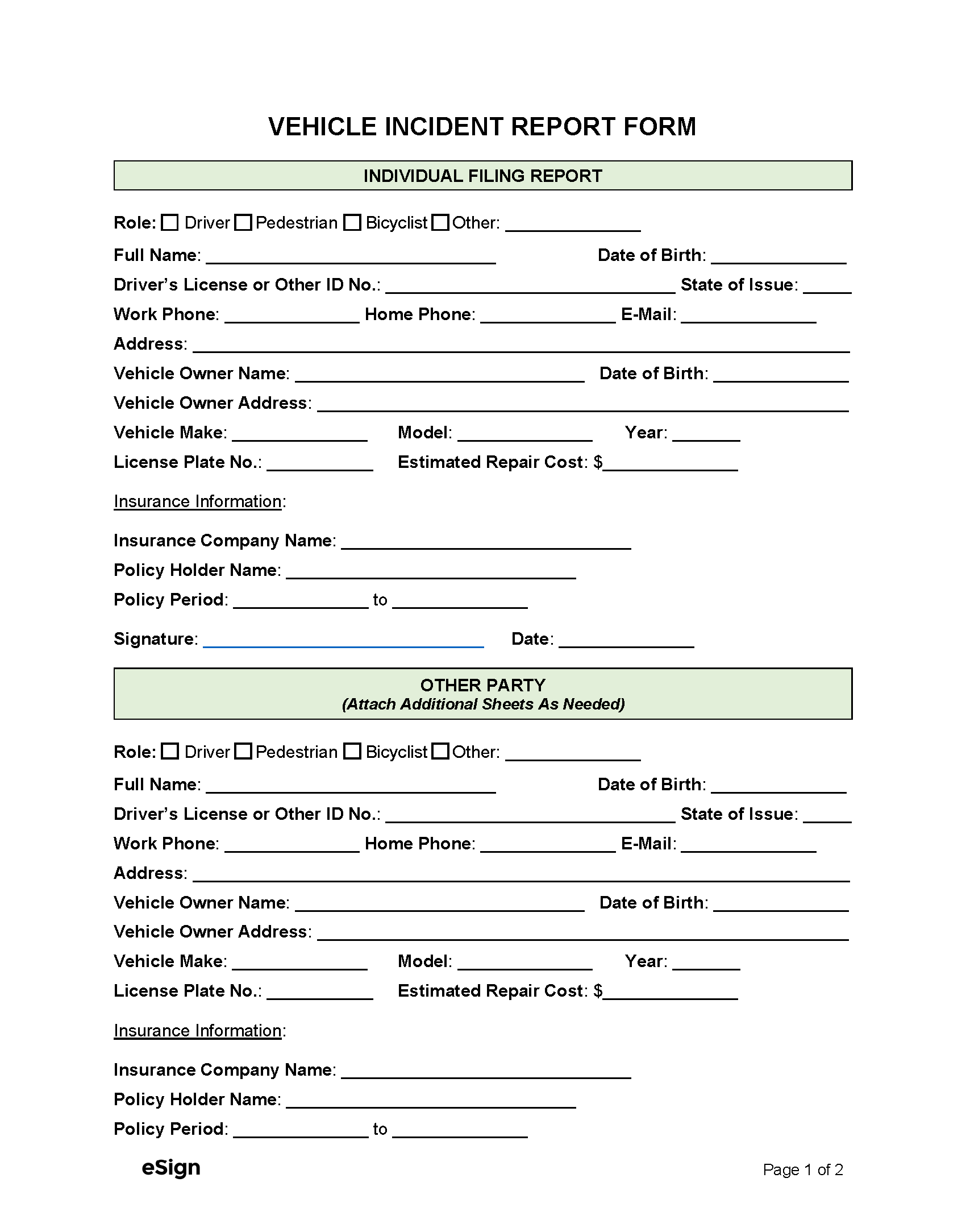
- Vehicle – Car crashes and damage to company vehicles.
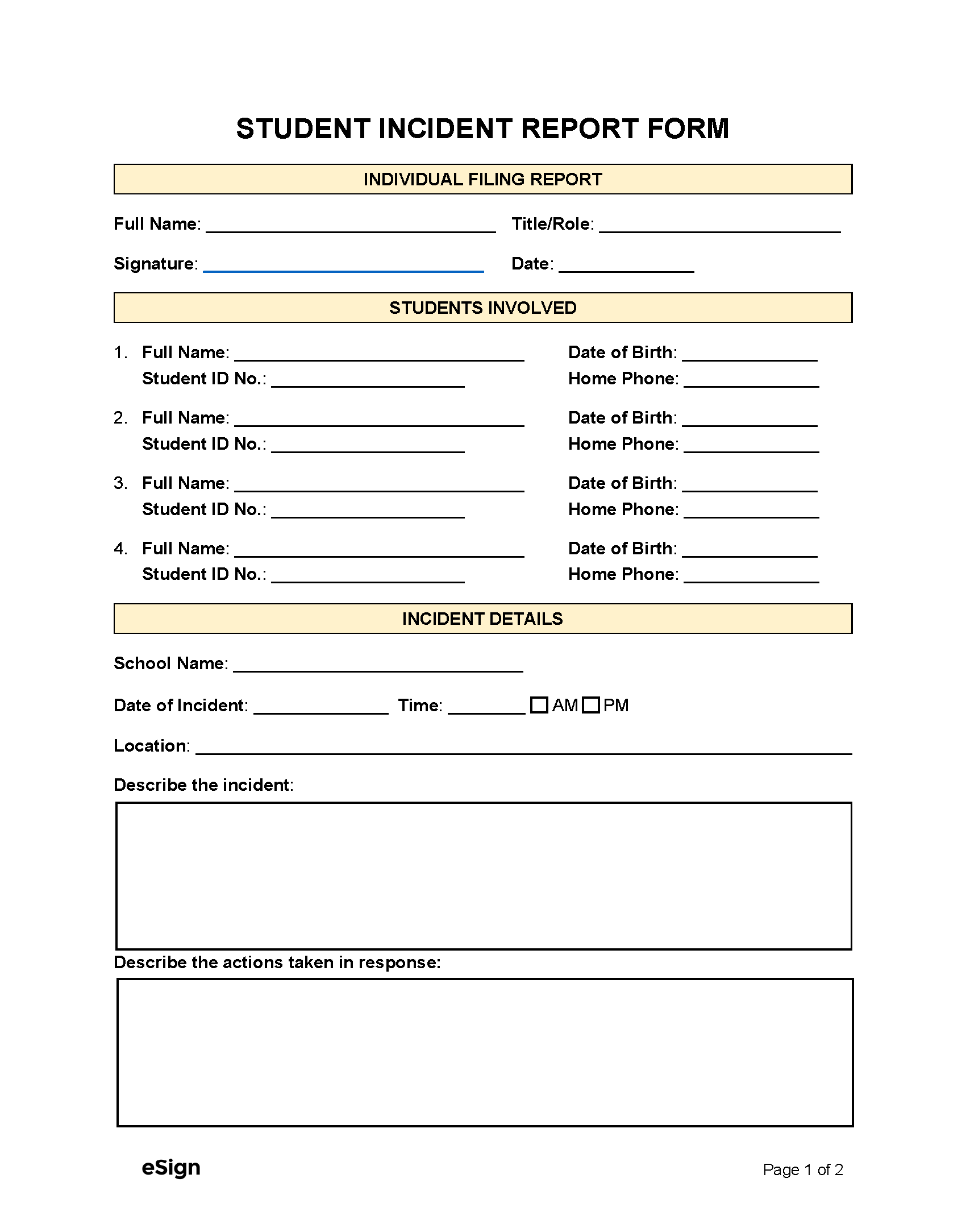
- School – Slips and falls on school property, student bullying, and sudden illnesses.
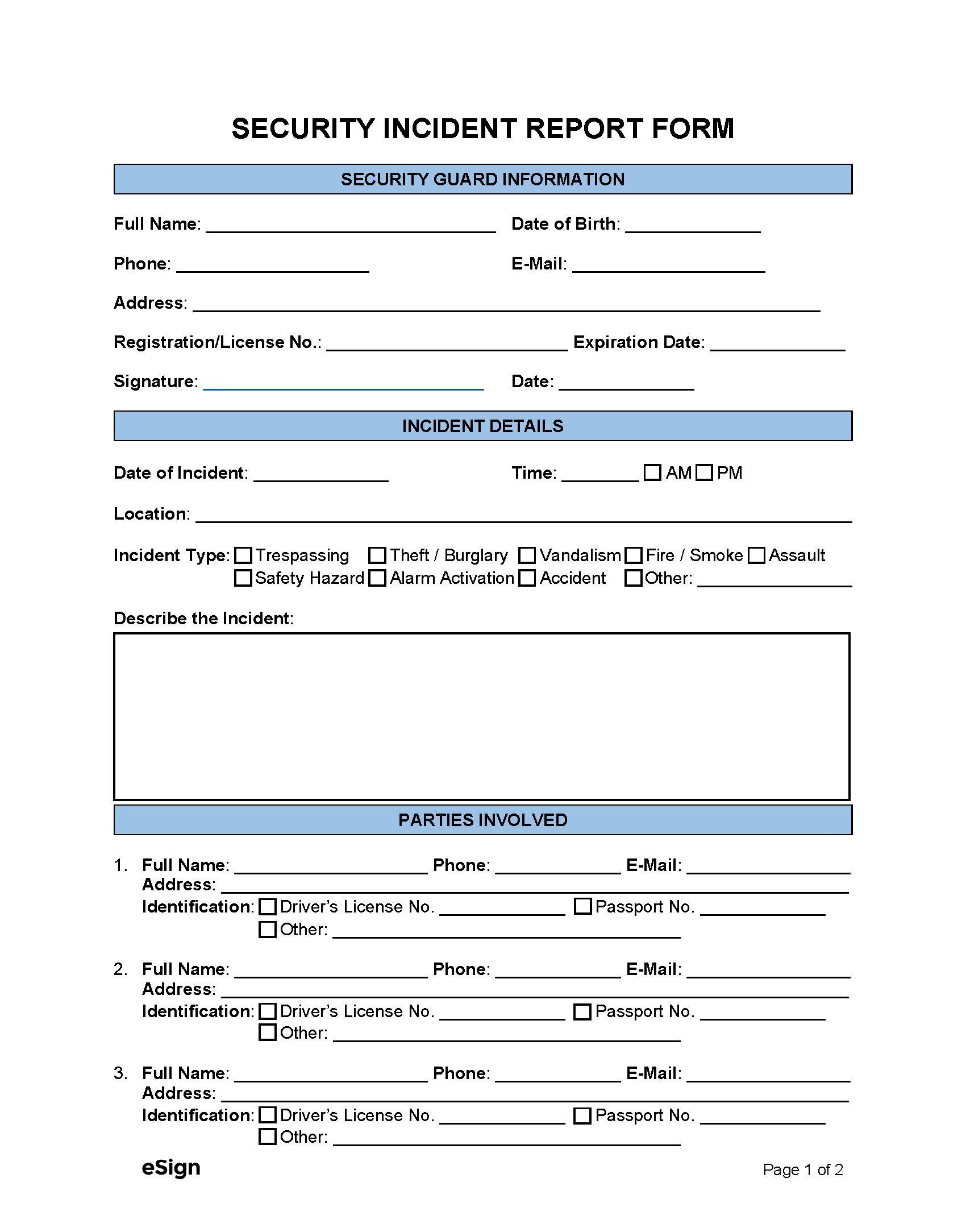
- Security – Stolen property, suspicious activity, cybersecurity attacks, and fire alarms.
- Medical Facility – Medication errors, aggressive behavior, and privacy breaches.
How to Write an Incident Report
If a person is involved in an incident, they should take the following steps to ensure their report is accurate and complete:
- Mention when and where the incident happened, who was involved, and provide any supporting evidence.
- Use clear, factual language without adding opinions.
- Record events in the order they occurred so the sequence is clear and easy to follow.
- Describe in detail any injuries or property damage.
- Finalize the document by signing and entering the date.
Supporting evidence, such as witness statements and photographs, should be attached. The completed report should then be submitted to the proper authority, which could be the HR department, law enforcement, or the DMV, depending on the situation.
By Type (17)

Sample
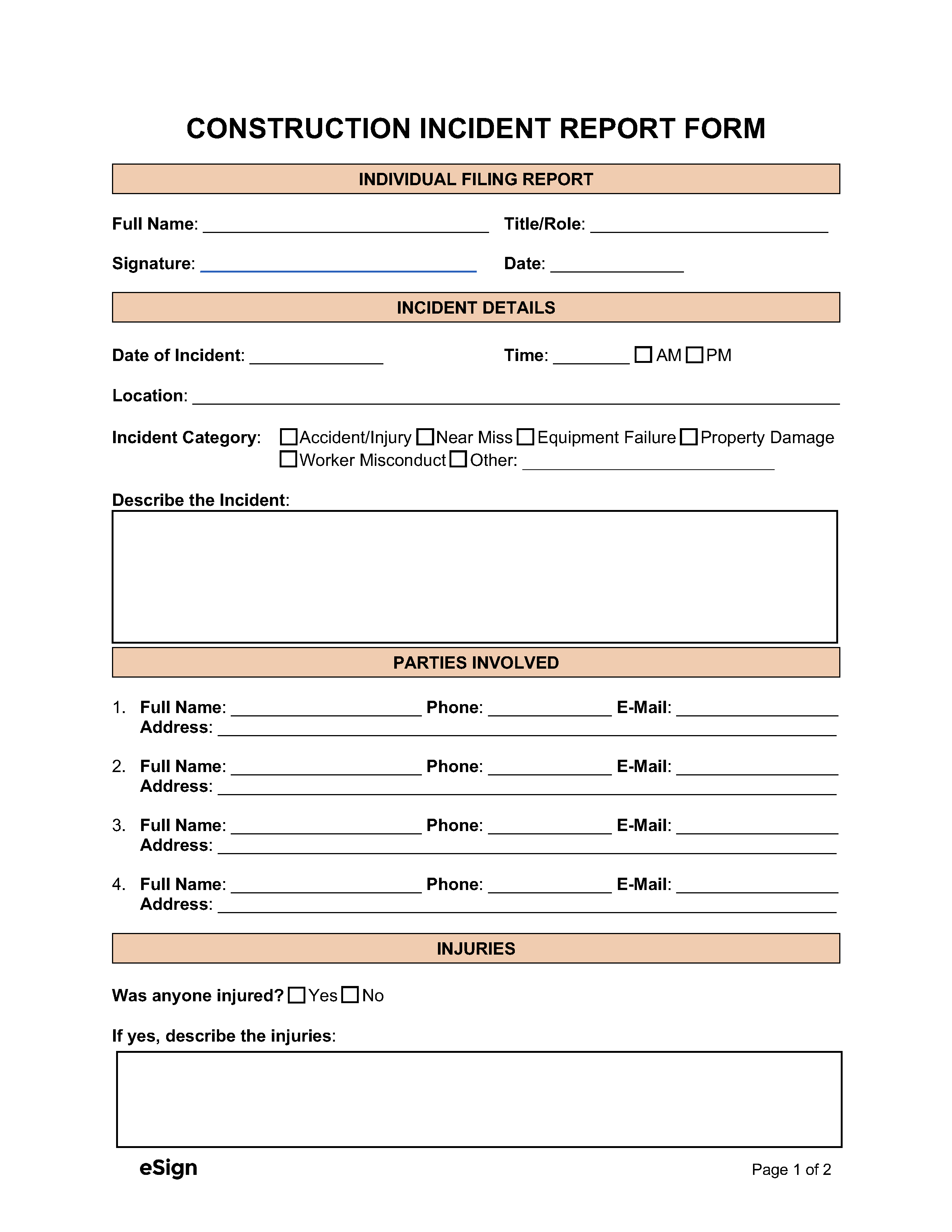
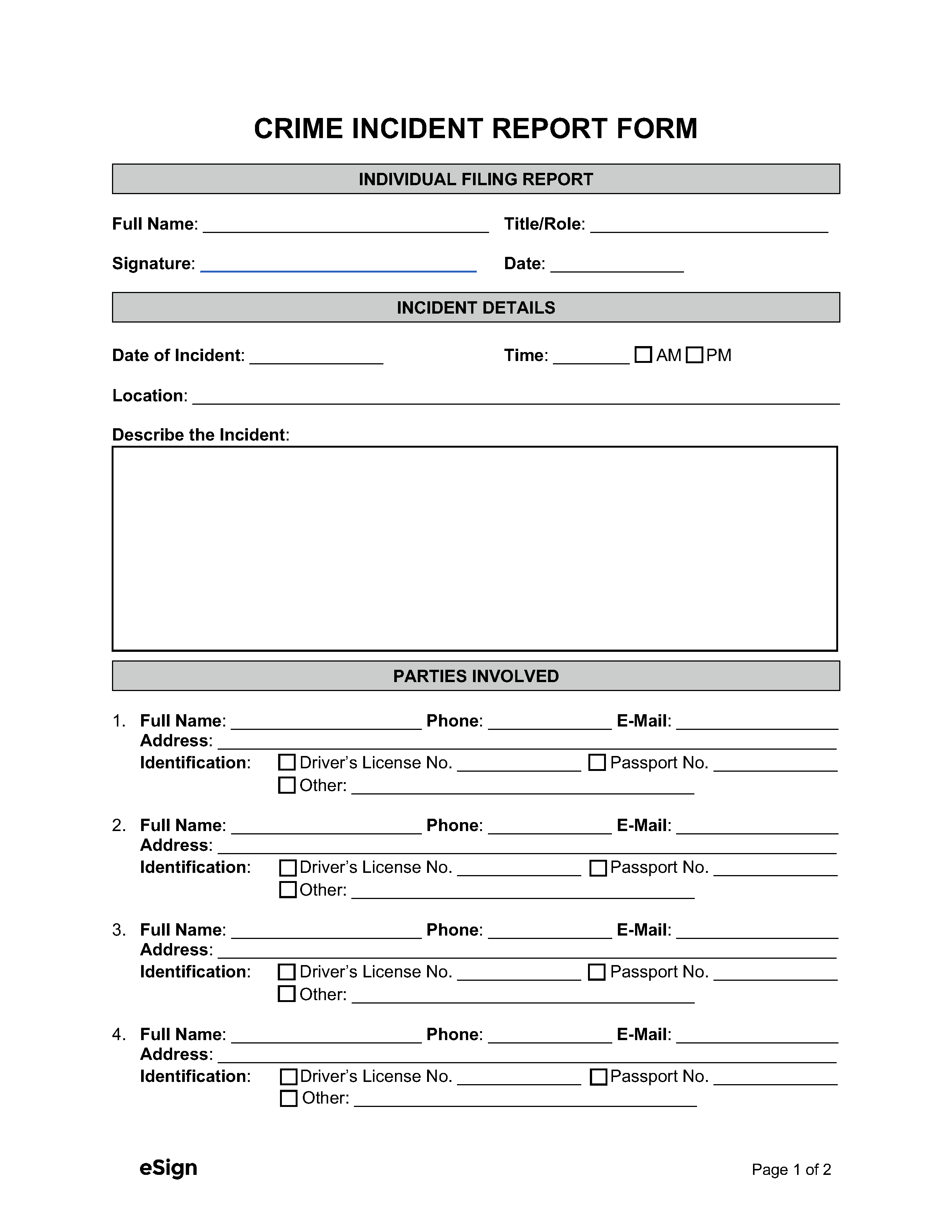
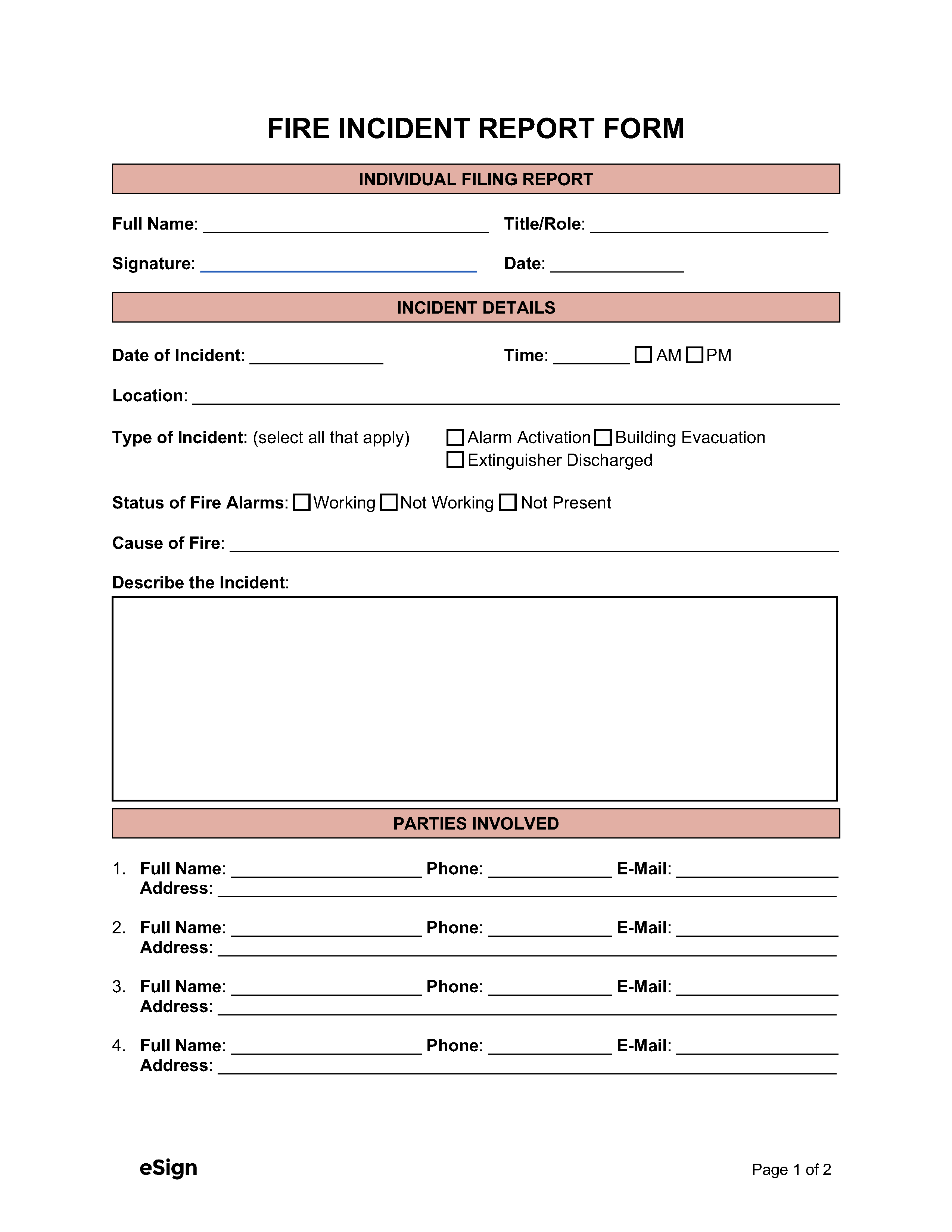
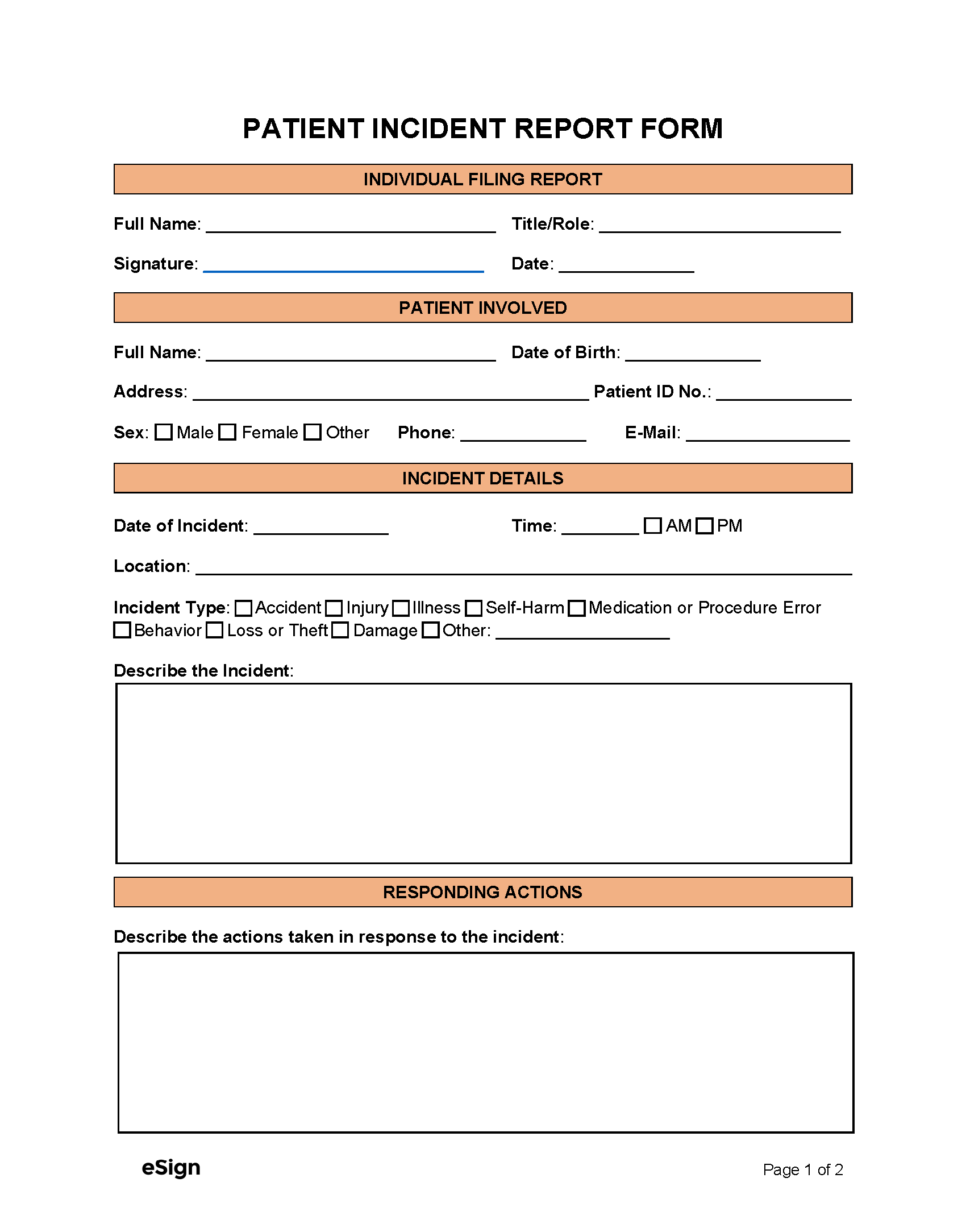
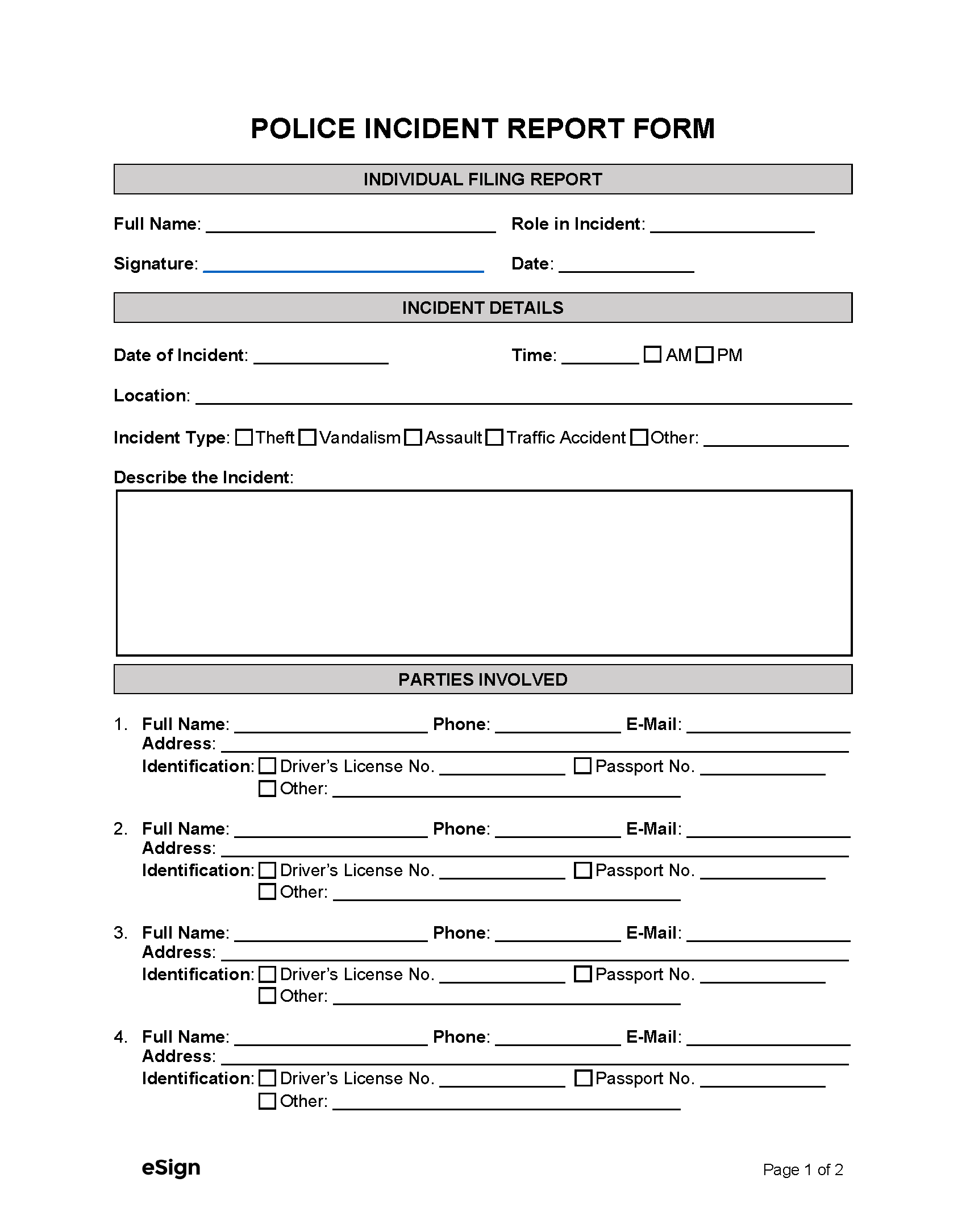
INDIVIDUAL FILING REPORT
Full Name: [FULL NAME] Title/Role: [TITLE/ROLE]
Signature: Date: [MM/DD/YYYY]
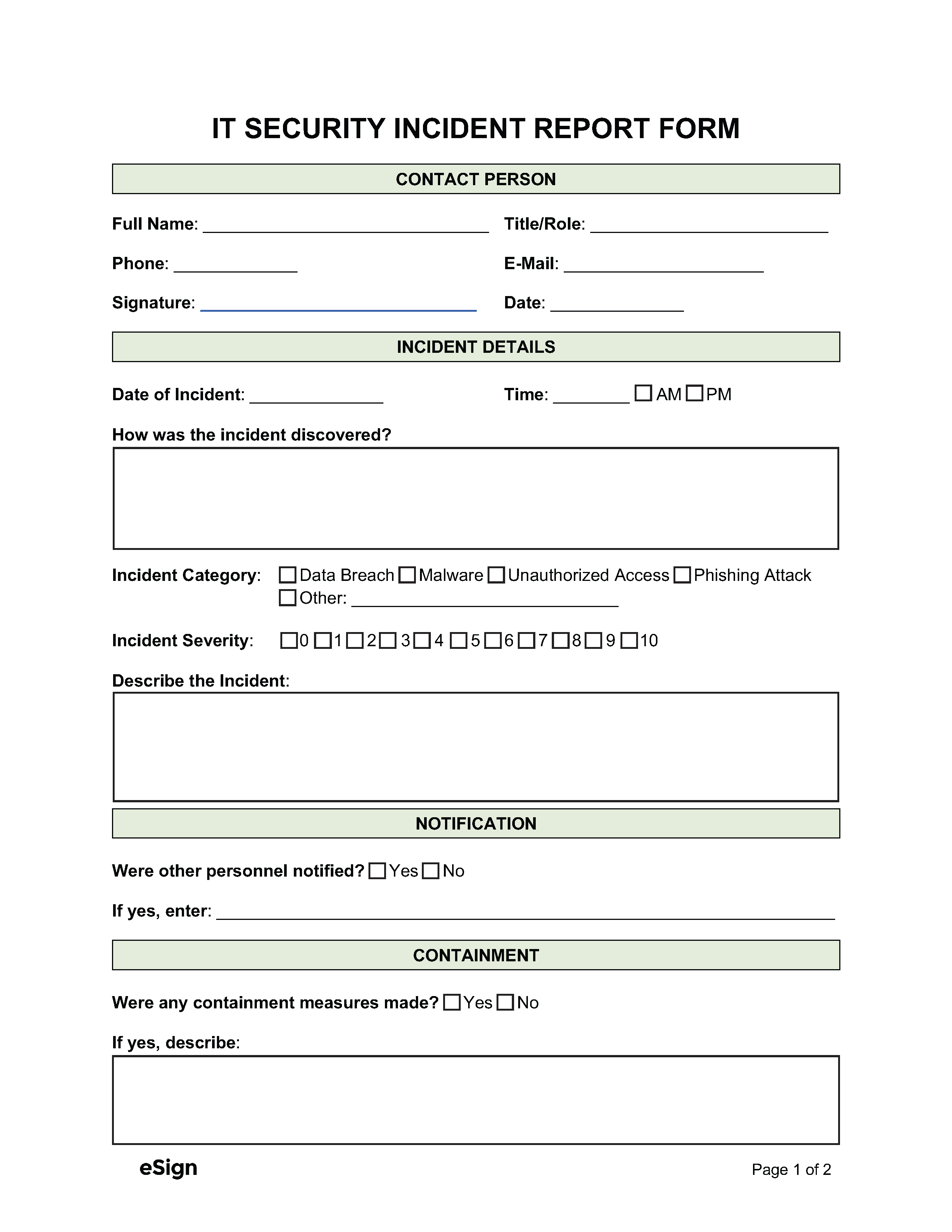
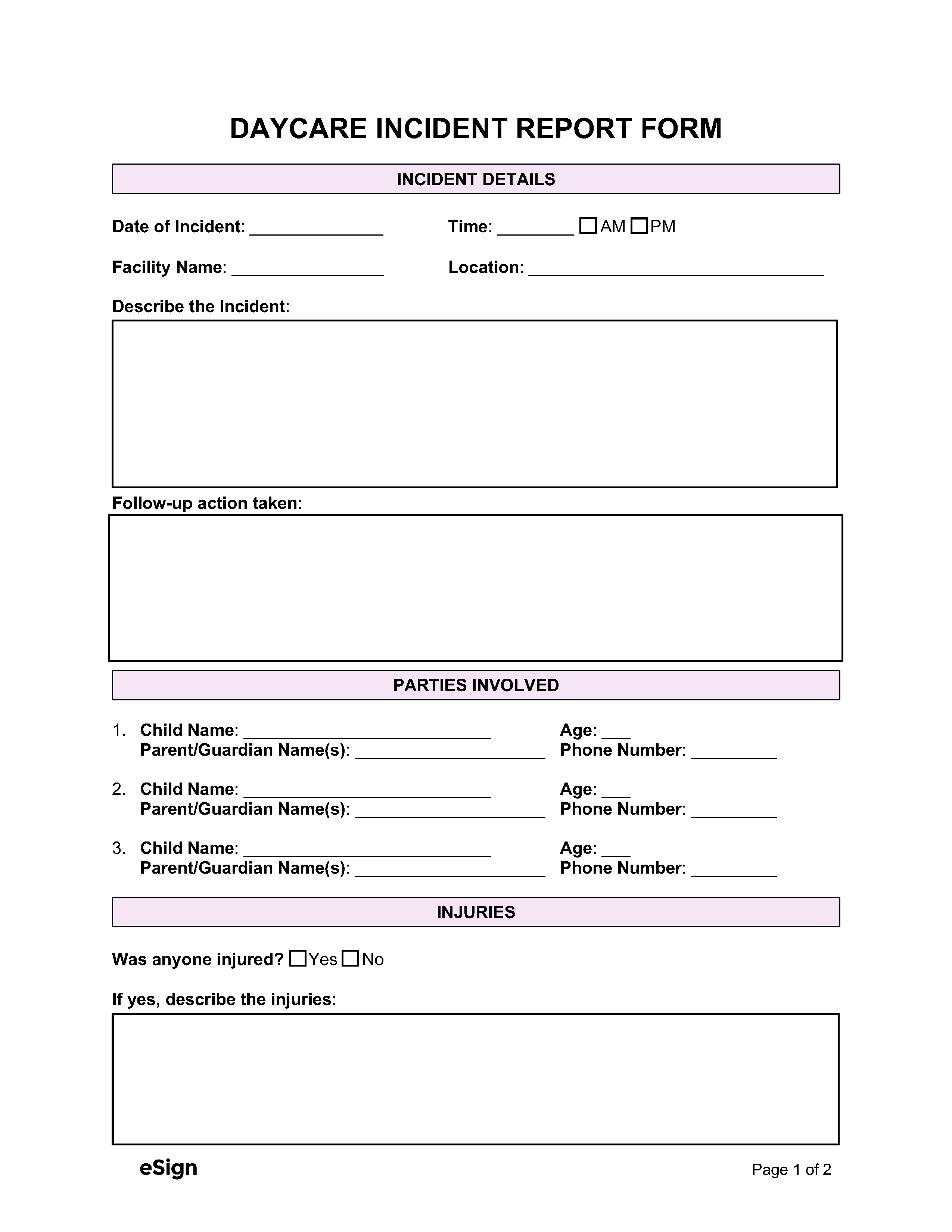
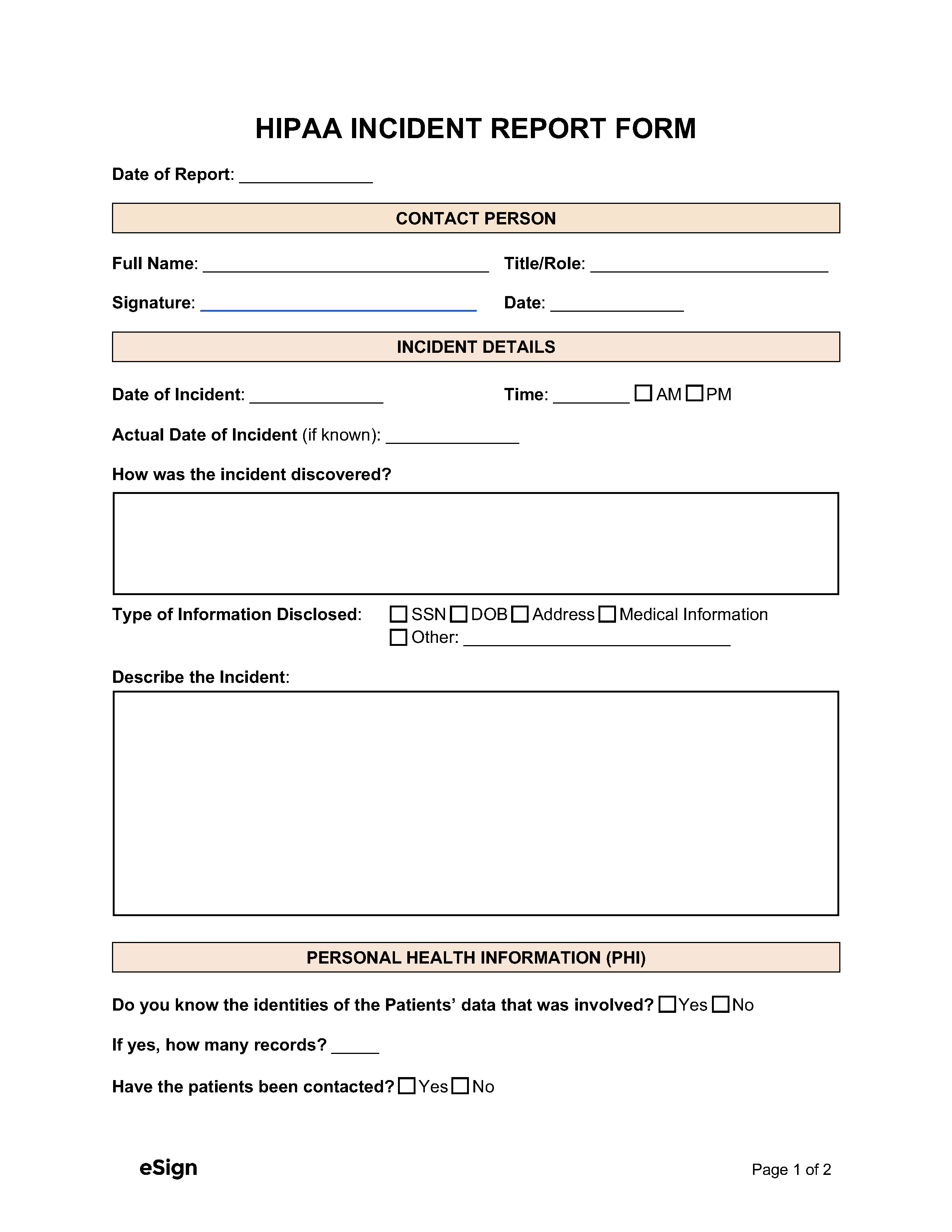
INCIDENT DETAILS
Location: [LOCATION]
Describe the Incident: [DESCRIBE THE INCIDENT]
- Full Name: [NAME] Phone: [PHONE] E-Mail: [E-MAIL] Address: [ADDRESS]
- Full Name: [NAME] Phone: [PHONE] E-Mail: [E-MAIL] Address: [ADDRESS]
- Full Name: [NAME] Phone: [PHONE] E-Mail: [E-MAIL] Address: [ADDRESS]
- Full Name: [NAME] Phone: [PHONE] E-Mail: [E-MAIL] Address: [ADDRESS]
INJURIES
Was anyone injured? ☐ Yes ☐ No
If yes, describe the injuries: [INJURY DESCRIPTION]
WITNESSES
Were there witnesses to the incident? ☐ Yes ☐ No
If yes, enter the witnesses’ names and contact info:
- Full Name: [FULL NAME] Phone: [PHONE] E-Mail: [EMAIL]
- Full Name: [FULL NAME] Phone: [PHONE] E-Mail: [EMAIL]
- Full Name: [FULL NAME] Phone: [PHONE] E-Mail: [EMAIL]
POLICE / MEDICAL SERVICES
Police Notified? ☐ Yes ☐ No
If yes, was a report filed? ☐ Yes ☐ No
Was medical treatment provided? ☐ Yes ☐ No ☐ Refused
If yes, where was medical treatment provided? ☐ On site ☐ Hospital ☐Other: [OTHER]